Arthroscopic Assisted Core Decompression of the Hip
Arthroscopic Assisted Core Decompression of the Hip
Arthroscopic Treatment of Avascular Necrosis (AVN) of the Femoral Head
While arthroscopy has been available to the orthopaedic community since its development in 1931, hip arthroscopy has only recently become popularized. A growing number of indications for hip arthroscopy has caused the number of procedures to increase eighteen-fold between 1999 and 2009.4 Current indications for hip arthroscopy include symptomatic loose bodies, labral lesions, femoral acetabular impingement (FAI), acute articular injury, traumatic rupture of the ligamentum teres, instability, peritrochanteric disorders (snapping hip, bursitis, gluteus medius tears), and joint sepsis.2 Yet another indication for hip arthroscopy is arthroscopic-assisted core decompression for avascular necrosis (AVN) of the femoral head.
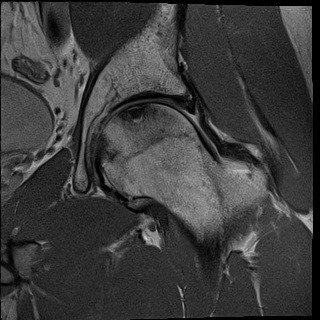
Osteonecrosis of the femoral head is a common condition with up to 20,000 new cases annually, accounting for about 10% of all total hip replacements. Patients with osteonecrosis of the femoral head present with symptoms at an average age of 38 years and typically experience an insidious onset of deep throbbing groin or lateral hip pain. The age of onset of symptoms and hip pain can be nearly identical to patients who experience symptomatic FAI and labral tears. In fact, MRIs of patients who are being worked up for FAI and labral pathology can occasionally reveal a silent, pre-collapse osteonecrosis of the femoral head (Picture 1). The presence of concomitant FAI and labral pathology in a patient with early stage AVN certainly confounds the situation. Is it the labral pathology that needs to be treated or the osteonecrosis? Physical exam maneuvers are not specific enough for these hip conditions to dictate whether it is the AVN that needs to be treated or the FAI. Hip arthroscopy gives us the potential to treat both types of pathology at the same time.
Avascular necrosis of the femoral head is associated with many conditions which all converge on a single common pathway: collapse of the femoral head and subsequent degenerative joint disease. These conditions include trauma, corticosteroid use, excessive alcohol consumption, systemic lupus erythematosus, sickle cell disease, renal failure or transplant, HIV, coagulopathies, connective tissue diseases, and Gaucher disease. Through mechanical interruption of blood flow, thrombosis/embolism, increased vascular pressure, or venous obstruction, essential blood flow to the femoral head is compromised leading to necrosis and inevitable collapse.
Core decompression of the femoral head has been utilized as a way to delay or prevent the need for hip arthroplasty in patients with early stages of AVN. While many theories have been formulated for why core decompression can be effective, the most accepted theory is that the formation of a core tract allows a drop in marrow pressure, which may reinstitute normal blood flow and allow new bone formation. In precollapse stages (0-II by Ficat5 and 0-III by Steinberg et al. staging methods), core decompression of the femoral head has been shown to be successful both clinically and radiographically when compared to nonoperative treatments.
Core decompression for osteonecrosis of the femoral head can be effectively performed with hip arthroscopy. In addition, the technique provides a method to address both the AVN and coexistent hip disorders in the same operation – namely labral pathology and cam and pincer lesions associated with FAI.
Figure 1. MRI of the Hip showing AVN of the femoral head without collapse